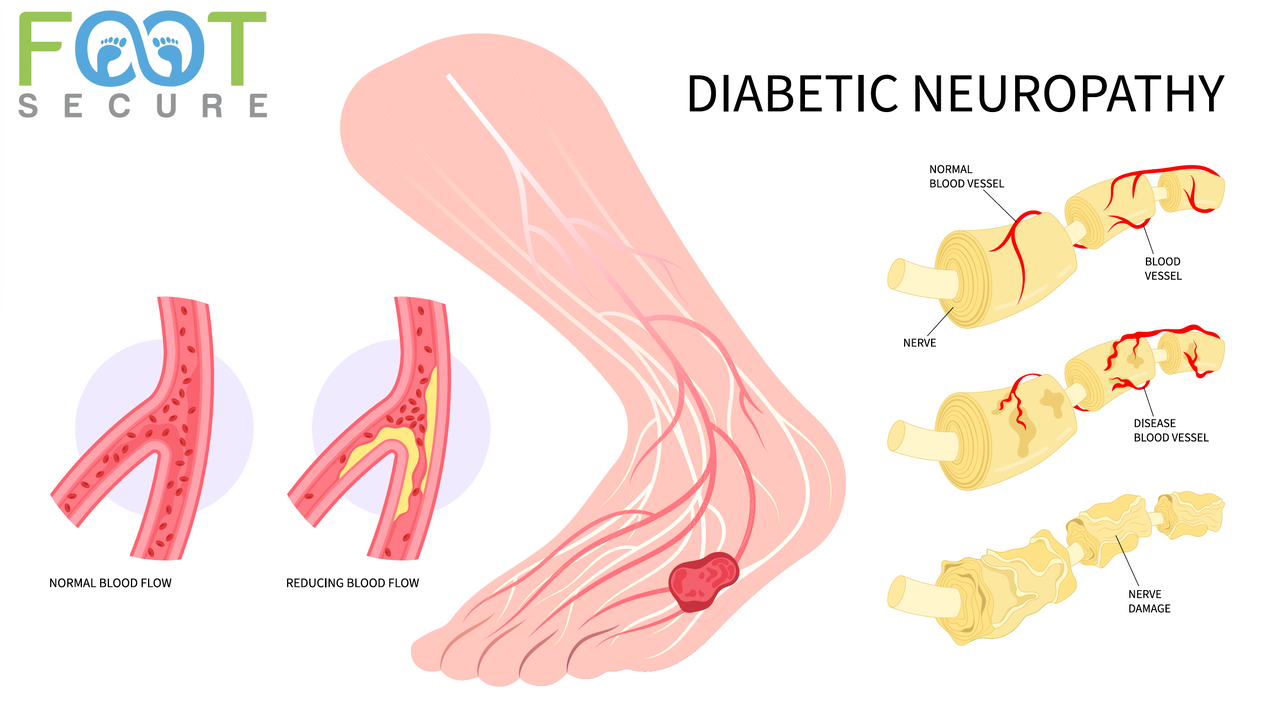
Diabetic neuropathy is defined as a nerve-damaging, neurodegenerative disorder of the peripheral nervous system, arising from chronic hyperglycemia and metabolic disturbances in diabetes patients, excluding other causes. It presents primarily as symmetric sensory-motor polyneuropathy (distal symmetrical polyneuropathy) or autonomic dysfunction, often affecting long axons first (feet). It is a chronic complication of diabetes characterized by injury to sensory, motor, and autonomic nerve fibers, leading to nerve fiber loss.

The International Diabetes Federation (IDF) and others classify it into four main types:
- Peripheral Neuropathy: Affects feet/legs (most common), and sometimes hands/arms.
- Autonomic Neuropathy: Affects involuntary functions (e.g., digestion, heart rate, bladder).
- Proximal Neuropathy (Diabetic Amyotrophy): Causes severe pain in thighs, hips, or buttocks.
- Focal Neuropathy: Causes sudden weakness or pain in specific nerves.
- Numbness or Reduced Sensation: A loss of feeling, often described as a "stocking-and-glove" distribution (starting in the toes/feet and sometimes hands), which can make it hard to feel temperature or pain.
- Tingling or "Pins and Needles": A tingling or prickling sensation in the hands or feet, often referred to as paresthesia.
- Burning or Sharp Pain: Intense burning, stabbing, throbbing, or shooting pains, which are often worse at night.
- Muscle Weakness: Weakness in the legs, feet, or hands, which can lead to difficulty walking, lifting the front part of the foot (foot drop), or dropping items.
- Extreme Sensitivity to Touch: A condition called hyperesthesia, where even the light weight of bedsheets can feel painful or uncomfortable.
- Digestive Issues: Symptoms of autonomic neuropathy, including chronic constipation, diarrhea, nausea, vomiting, or feeling full after only a few bites of food (gastroparesis).
- Dizziness or Lightheadedness: Low blood pressure upon standing (orthostatic hypotension), causing a sudden drop in pressure that leads to dizziness.
- Foot Problems: Development of calluses, sores, or ulcers on the feet due to lost sensation, which may not be felt immediately, leading to risk of infection.
Diabetic neuropathy stems from chronic hyperglycemia causing metabolic, vascular, and inflammatory damage to peripheral nerves. Key mechanisms include increased polyol pathway activity (sorbitol accumulation), oxidative stress, advanced glycation end-products (AGEs) formation, and microvascular insufficiency, leading to segmental demyelination, axonal degeneration, and impaired nerve regeneration.

- Metabolic Factors (Hyperglycemia): High glucose levels drive excess glucose into the polyol pathway, reducing nicotinamide adenine dinucleotide phosphate (NADPH) and causing accumulation of sorbitol. This creates oxidative stress and reduces Na+/K+-ATPase activity, disrupting nerve conduction.
- Microvascular Dysfunction: Chronic hyperglycemia causes damage to the small blood vessels (vasa nervorum) that supply nerves, leading to hypoxia (lack of oxygen) and ischemia.
- Advanced Glycation End-products (AGEs): Increased glucose leads to the nonenzymatic glycation of proteins, forming AGEs. These products bind to receptors (RAGE), triggering inflammatory responses, vascular dysfunction, and neuronal apoptosis.
- Protein Kinase C (PKC) Activation: Hyperglycemia increases PKC activation, which contributes to decreased nerve blood flow, increased vasoconstriction, and vascular permeability.
- Neurotrophic Support Deficit: Reduced insulin signaling and neurotrophic factors (nerve growth factors) impair the ability of neurons to repair themselves, resulting in nerve damage.
These metabolic and vascular changes result in:
- Segmental demyelination: Damage to the myelin sheath covering nerves.
- Axonal degeneration: Breakdown of the nerve fiber itself, often starting distally (longest nerves first).
Physiotherapy assessment of diabetic neuropathy focuses on evaluating sensory loss, motor weakness, and balance deficits to prevent falls and foot ulcers. Key assessments include checking sensation, strength, gait, and skin integrity to create a tailored exercise and protection plan. Key assessments include:
- Monofilament Testing (10-g): Evaluates protective sensation at specific points on the foot to identify high-risk areas.
- Vibration Perception Test: Uses a tuning fork (128 Hz) to test deep sensory perception, often lost early in neuropathy.
- Balance and Fall Risk Assessment: Uses scales like the Berg Balance Scale or Timed Up and Go (TUG) to evaluate instability.
- Muscle Strength Testing (Manual Muscle Test): Assesses for atrophy and weakness in lower limb muscles (e.g., ankle dorsiflexors, toe flexors).
- Joint Mobility and Flexibility Assessment: Measures range of motion in ankles and toes, looking for stiffness like cheiroarthropathy.
- Gait Analysis: Evaluates walking patterns to identify deviations caused by weak muscles or lack of sensation.
- Skin and Footwear Assessment: Inspects for signs of irritation, calluses, or ulcers and evaluates if shoes are protective and fit properly.
- Pain Assessment (Neuropathic Scales): Evaluates burning, tingling, or numbness to measure intensity and impact on function.
PHYSIOTHERAPY

Physiotherapy for diabetic neuropathy aims to reduce pain, improve balance, prevent falls, and increase functional mobility through targeted exercises and modalities. Key interventions include tailored aerobic activity, strength training, balance training, gait training, sensory re-education, and pain-relieving techniques like TENS or laser therapy.
- Aerobic Exercise: Low-impact activities such as walking, cycling, or swimming improve cardiovascular health, reduce blood glucose levels, and improve nerve function.
- Strength Training: Progressive resistance exercises, particularly for the lower extremities (e.g., ankle dorsiflexion, heel raises), help manage muscle weakness associated with peripheral neuropathy.
- Balance Training: Techniques like Tai Chi, single-leg stance, and wobble board exercises are crucial for reducing fall risk due to reduced sensory feedback.
- Gait Training: Exercises focusing on walking patterns, including tandem walking or stepping over obstacles, improve proprioception and confidence in mobility.
- Flexibility Exercises: Regular, gentle stretching of the calves and hamstrings helps prevent contractures and reduces muscle stiffness, improving mobility in the feet and legs.
- Transcutaneous Electrical Nerve Stimulation (TENS): TENS is used to manage neuropathic pain by applying low-voltage electrical currents to the skin, which can reduce pain sensations.
- Sensory Re-education: Techniques that help the brain re-interpret signals from the feet, such as using different textures to rub on the skin, help manage numbness and tingling.
- Balance and Foot Care Exercises: Daily exercises such as seated toe raises, ankle pumps, and walking exercises help maintain foot function and increase blood circulation.
9.Other supportive interventions include massage therapy (e.g., Thai foot massage) for circulation and comfort, and the use of orthotics or splints (e.g., ankle-foot orthoses) to support weak joints and prevent injuries.