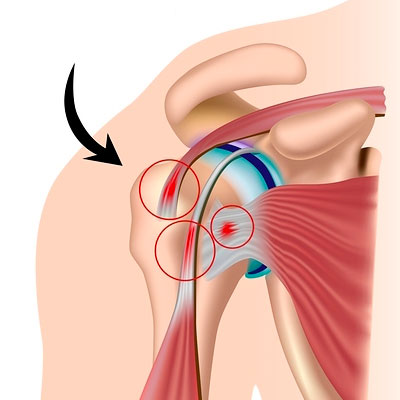
Shoulder impingement syndrome (SIS) is caused by the compression of rotator cuff tendons and the subacromial bursa against the acromion during overhead arm movements, typically due to narrowed subacromial space. It involves extrinsic mechanical impingement (hooked acromion, bone spurs) or intrinsic degenerative changes in the tendon itself. This compression leads to a cycle of inflammation, tendinopathy, and potential tears.
Key Pathophysiological Mechanisms:
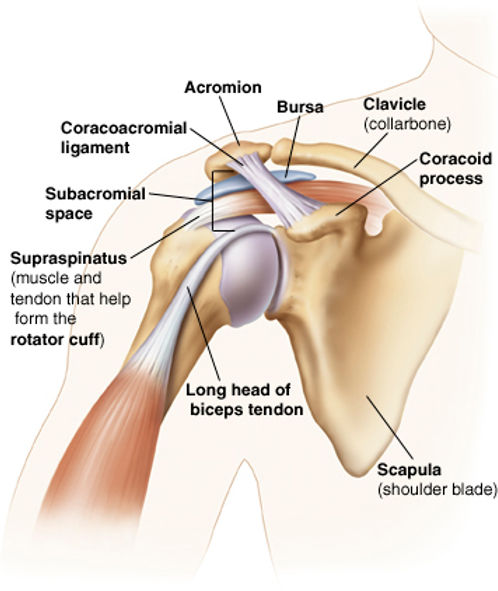
- Subacromial Space Narrowing (Extrinsic Impingement): This is the most common cause, where the subacromial space (normally 7–14 mm) is reduced, creating a mechanical conflict between the rotator cuff and superior structures (acromion, CA ligament).
- Acromial Morphology: A curved (Type II) or hooked (Type III) acromion, defined by Bigliani et al., can physically grind against the tendon.
- Acromioclavicular (AC) Joint Arthrosis: Osteophytes (bone spurs) forming under the AC joint reduce space.
- Thickening of Structures: Subacromial bursitis (bursal thickening) and thickening of the coracoacromial (CA) ligament reduce space.
- Intrinsic Degeneration (Rotator Cuff Tendinopathy): Age-associated degeneration and decreased vascular supply to the rotator cuff tendon (specifically the supraspinatus) reduce its structural integrity, making it more prone to damage under normal loading.
- Biomechanical Factors and Instability:
- Scapular Dyskinesis: Suboptimal scapular movement reduces subacromial clearance.
- Internal Impingement: A distinct form often seen in overhead athletes where the undersurface of the rotator cuff compresses against the posterior-superior glenoid rim.
- Glenohumeral Instability: Improper seating of the humeral head forces it to glide too high, pinching the rotator cuff.

Progression of Pathology:
- Inflammation and Edema: Initial irritation of the bursa and rotator cuff (often in younger patients, <25).
- Tendinopathy and Fibrosis: Recurrent irritation causes structural changes and thickening in the tendon and bursa.
- Partial/Full Thickness Tears: Chronic abrasion leads to tear formation.
Here are the clinical features commonly observed in shoulder impingement syndrome:
- Anterolateral Shoulder Pain: Pain often presents at the front and outer side of the shoulder, frequently radiating down to the mid-humerus, particularly when lifting the arm or sleeping on it.
- Painful Arc of Motion: A sharp, stabbing pain commonly occurs when moving the arm actively between 70° and 120° of abduction (lifting the arm out to the side).
- Nocturnal Pain & Difficulty Sleeping: Patients often complain of pain that breaks their sleep, specifically making it difficult to lie on the affected shoulder.
- Positive Impingement Signs: Physical tests, such as the Hawkins-Kennedy test (internal rotation with arm at 90°) and the Neer test (passive forward flexion), produce significant pain.
- Weakness in Overhead Movements: Weakness is often experienced during shoulder abduction or external rotation, usually caused by pain inhibition (pain-limited weakness), particularly when lifting objects above head level.
- Reduced Range of Motion (Stiffness): A general decrease in range of motion, which interferes with daily activities like brushing hair, reaching into a back pocket, or dressing.
Key Special Tests for Shoulder Impingement
- Hawkins-Kennedy Test: With the patient's arm at 90° forward flexion and elbow at 90°, the examiner passively rotates the arm internally. Pain indicates a positive test.
- Neer Test: The examiner stabilizes the scapula, then performs passive maximal forward flexion of the arm in internal rotation. Pain indicates a positive result.
- Painful Arc Test: The patient actively abducts the arm in the scapular plane, noting pain between roughly 60°–120°. Pain in this range indicates a positive test.
- Empty Can Test (Jobe's Test): The shoulder is abducted to 90° and internally rotated (thumb pointing down). The patient resists downward pressure by the examiner.
- External Rotation Resistance Test: With the elbow at 90° and tucked in at the side, the patient resists internal rotation (or the examiner resists external rotation).

Here are 8 common physiotherapy interventions:
- Pendulum Exercises (Codman's): Relieves pain by gently increasing space in the joint, performed by leaning forward and swaying the arm in small circles or motions.
- Scapular Squeezes (Retraction): Improves posture and shoulder blade stability by squeezing shoulder blades together.
- Isometric Shoulder Rotation (Internal/External): Builds strength without moving the joint, often done by pushing against a wall with a bent elbow.
- Side-Lying External Rotation: Strengthens the rotator cuff by lying on the non-injured side and lifting a light dumbbell or rotating against band resistance.
- Wall Angels: Improves mobility and posture by standing against a wall and moving arms up and down like a snow angel.
- Resistance Band Row/Pull Down: Targets posterior shoulder muscles and scapular stabilizers, strengthening the muscles that support the shoulder.
- Supported Overhead Stretches: Using a stick or the healthy arm to lift the affected arm, increasing range of motion.
- Chest/Pectoral Stretch: Opens the chest to correct rounded shoulders that restrict the subacromial space.
- Soft tissue manipulation,heat therapy,TENS Therapy and ultrusound Therapy.