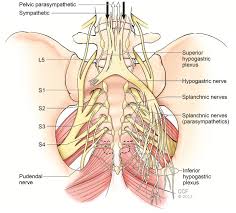
Maternal obstetric palsy (or obstetric maternal lumbosacral plexopathy) is a rare neurological injury occurring during or after labor, characterized by damage to the lumbosacral plexus due to compression. It causes sensory and motor dysfunction, including lower-limb pain, weakness, numbness, or foot drop. 
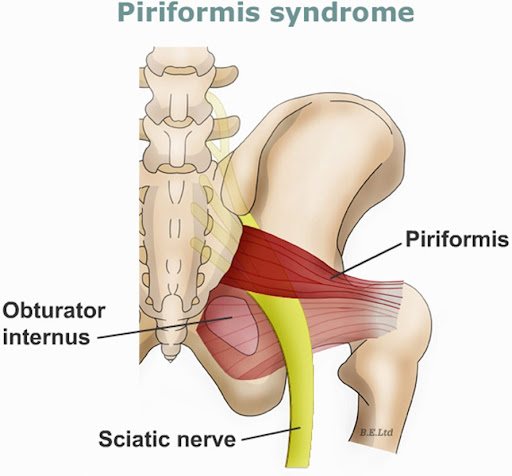
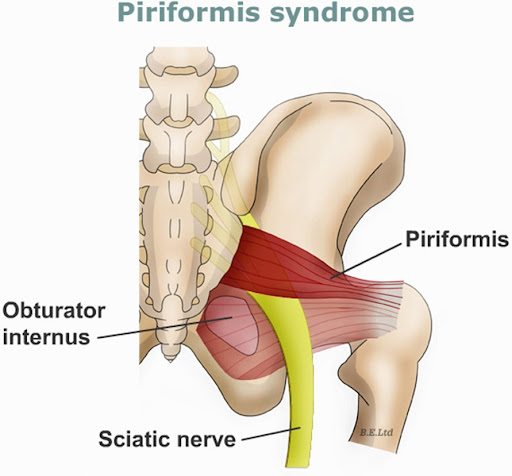
- Compression: The fetal head, particularly in cephalopelvic disproportion, compresses the lumbosacral trunk against the sacral ala and pelvic brim.
- Ischemia: The intense pressure compromises blood supply to the nerves, leading to ischemia and subsequent nerve dysfunction.
- Segmental Demyelination: The structural damage often presents as segmental demyelination.
- Nerve Involvement: The lumbosacral trunk is particularly vulnerable, often causing damage to the peroneal nerve (causing foot drop).
- Foot Drop: Weakness of ankle dorsiflexion, making it difficult to lift the front part of the foot.
- Pain and Paresthesia: Pain and sensations of tingling or "pins and needles" in the affected limb.
- Motor Weakness: Weakness in ankle eversion and inversion.
- Sensory Loss: Numbness, often following the L5/S1 nerve root distribution (back of thigh, calf, or foot).
- Sensori-neuropathy: Perineal sensations might be impaired.
- Gait Disturbance: Difficulty walking or steppage gait due to weakness.
- Muscle Wasting: Atrophy of the muscle groups in the lower leg (if the injury is chronic/severe).
- Reflex Deficits: Diminished or absent knee or ankle jerk reflexes.
- Labor Mechanics: Prolonged or difficult second stage of labor often leads to this condition, usually due to pressure from the fetal head on the lumbosacral plexus.
- Cephalopelvic Disproportion (CPD): A mismatch between the fetal head size and the maternal pelvic capacity.
- Macrosomia/Large Fetus: A high-weight baby increases the likelihood of pelvic pressure.
- Fetal Malposition: Abnormal position of the fetus during delivery.
- Instrumental Delivery: Use of mid-forceps rotation increases the risk.
- Maternal Factors: Short stature (often defined as <150 cm) and primiparity (first pregnancy) are considered risk factors.
- Positioning: Long periods of maintained, static positions (e.g., extreme hip flexion/lithotomy position) during labor.
- Anesthesia: Spinal anesthesia is more frequently associated with this complication than epidural anesthesia.

- Neurological Examination: Assess motor strength (especially ankle dorsiflexors, inverters, and evertors), sensory loss in the lower extremities, and tendon reflexes.
- Gait Assessment: Evaluate for a high-stepping or "steppage" gait caused by foot drop.
- Muscle Power Testing: Evaluate ankle, knee, and hip strength to determine the extent of nerve damage.
- Functional Assessment: Assess the patient’s ability to walk, stand, and manage daily activities.
- Foot drop: Inability to lift the front part of the foot.
- Sciatic nerve-area pain: Pain and paresthesia in the lower extremity.
- Weakness/Paralysis: Involvement of the ankle, knee, or hip depending on the extent of the compression.
PHYSIOTHERAPY
Maternal obstetric palsy (MOP) physiotherapy focuses on relieving pain, preventing contractures, and restoring mobility after nerve compression during labor. Effective interventions include electrical stimulation, therapeutic exercises, and gait training to address lower limb motor/sensory deficits, usually starting with positioning to prevent further damage and progressing to strengthening.
- Transcutaneous Electrical Nerve Stimulation (TENS): Used to reduce severe pain and manage muscle spasms.
- Electrical Muscle Stimulation (EMS/FES): Applied to stimulate denervated muscles to prevent atrophy and improve function.
- Passive Range of Motion (PROM) Exercises: Performed in the early phase to maintain joint mobility and prevent contractures.
- Active-Assisted and Active Exercises: Progressive strengthening exercises for weak lower limb muscles.
- Isometric Muscle Exercises: Strengthening exercises initiated early to prevent muscle wasting without requiring significant joint movement.
- Proper Positioning/Splinting: Positioning limbs (e.g., hips in extension/slight abduction, knees extended) and using ankle-foot orthoses (AFOs) to prevent foot drop.
- Gait Retraining: Parallel bars, crutches, or walking aids to retrain walking mechanics, often addressing high-steppage gait.
- Proprioceptive/Coordination Training: Balance training to improve joint position awareness and stability, such as standing on uneven surfaces.
- Stretching Techniques: Targeted stretching to manage muscle contractures arising from nerve palsy.
- Pain Management Modalities: Including gentle heat or controlled cold (cryotherapy) to manage pain and spasm.