Total hip arthroplasty (THA) is a common, highly successful surgical procedure that replaces a damaged hip joint—typically due to arthritis or fracture—with an artificial prosthesis. It involves replacing both the femoral head (ball) and the acetabulum (socket) to relieve pain and improve mobility.

- Bones: The articulation is between the head of the femur and the acetabulum of the pelvis, which is composed of the ilium, ischium, and pubis.
- Articular Cartilage: Both surfaces are covered with hyaline cartilage to provide smooth motion.
- Acetabular Labrum: A fibrocartilaginous collar that deepens the acetabulum, increasing stability and sealing the joint.
- Joint Capsule & Ligaments: A strong, dense capsule strengthened by three primary extracapsular ligaments—the iliofemoral (strongest), pubofemoral, and ischiofemoral ligaments. The ligamentum teres is an intracapsular ligament that provides minor support.
- Muscles Acting on the Hip:
The hip is surrounded by powerful muscle groups, including:- Flexors: Iliopsoas, Rectus femoris.
- Extensors: Gluteus maximus, Hamstrings.
- Abductors: Gluteus medius, Gluteus minimus.
- Adductors: Adductor magnus, longus, brevis, and gracilis.
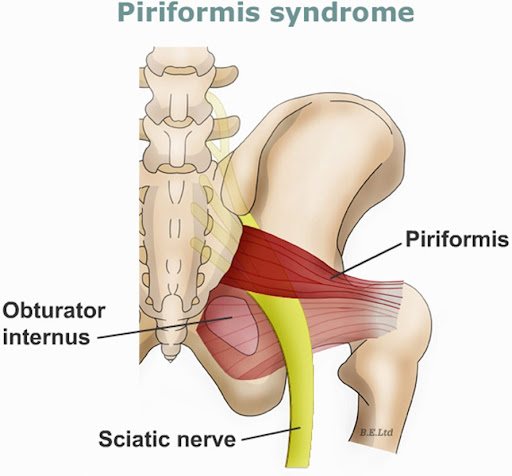
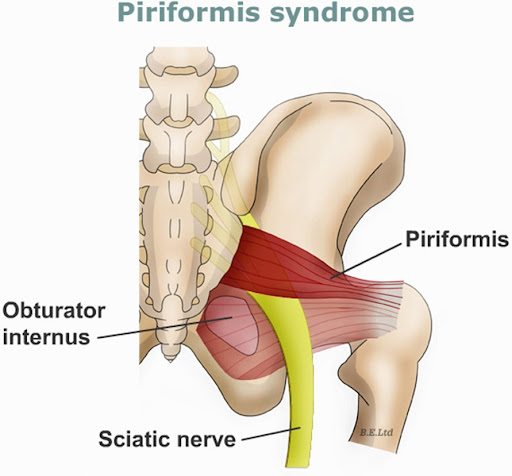
- Rotators: Deep rotators (piriformis, obturators) and gluteus maximus.
Blood Supply & Innervation:- Blood: Primarily supplied by the medial and lateral circumflex femoral arteries.
- Nerves: The joint is innervated by branches of the femoral, obturator, and sciatic nerves.
- Clinical Relevance:
The hip joint's structure is critical for supporting the weight of the body while allowing for locomotion, such as walking, running, and rotating. Key structures like the labrum and cartilage are common sites of injury, pain, and degeneration.
INDICATIONS
Total hip arthroplasty (THA) is indicated for patients with severe, chronic hip pain and functional impairment, usually due to osteoarthritis, that has failed to improve with conservative treatments (physical therapy, medication). Key indications include significant daily activity limitations, severe radiographic joint deterioration, femoral neck fractures, and avascular necrosis.
- Osteoarthritis (OA): The most common indication, characterized by wear-and-tear arthritis that causes loss of cartilage.
- Rheumatoid Arthritis (RA): Chronic inflammation that destroys the joint cartilage.
- Avascular Necrosis (AVN): Also known as osteonecrosis, involving the death of bone tissue in the femoral head, often leading to collapse.
- Post-traumatic Arthritis: Arising from severe hip injuries or fractures.
- Femoral Neck Fractures: Frequently in patients over 60 years old.
- Hip Dislocation: Residual impact on the joint.
- Tumors: Primary or metastatic tumors of the hip joint.
- Ankylosing Spondylitis: A chronic inflammatory disease.
- Failure of Non-Surgical Treatment: Initial treatments, such as medication, lifestyle changes, and physical therapy, have not provided relief.
- Persistent Pain: Chronic pain that limits daily activities (e.g., walking, bending).
- Reduced Quality of Life: Substantial limitation of movement and reduced independence.
PHYSIOTHERAPY MANAGEMENT
(A)Pre-Operative Physiotherapy
Filters and topics
- Educating the patient about post-operative precautions (e.g., avoiding excessive flexion, adduction, and internal rotation) and teaching them how to move safely in bed and perform transfers (sit-to-stand) to avoid hip dislocation.
- Lower Limb Strengthening Exercises
Targeting key muscle groups supporting the hip joint to improve post-operative stability. This includes strengthening the hip abductors, extensors, and knee extensors to help with early walking. - Gait Training and Assistive Device Education
Training the patient in the proper use of mobility aids (e.g., crutches or walkers) to ensure safe ambulation immediately after surgery, including instructions on partial weight-bearing if required. - Flexibility and Range of Motion (ROM) Exercises
Increasing the flexibility of muscles surrounding the hip joint (hip flexors, hamstrings) 6-8 weeks prior to surgery to reduce contractures and improve functional movement following the procedure. - Breathing Exercises and Respiratory Care
Teaching deep breathing techniques and incentive spirometry to prevent post-operative pulmonary complications (like pneumonia) due to anesthesia and bed rest. - Cardiovascular Endurance Training
Implementing moderate-intensity aerobic exercises, such as stationary cycling or walking, to improve cardiovascular fitness, and reduce the overall length of hospital stay. - Functional Activity Training (ADL Education)
Practicing functional tasks, such as stair climbing and proper bed mobility (getting in/out of bed) prior to surgery, to enhance the patient’s confidence and independence immediately post-op.
(B)Post Operative Physiothrapy
Post-operative physiotherapy for Total Hip Arthroplasty (THA) is essential for restoring mobility, preventing complications, and strengthening the surrounding musculature. Interventions typically begin on the day of surgery or the following day and progress through phases of recovery.
- Ankle Pumps and Circulatory Exercises: Performed early on, these exercises involve moving the feet up and down to increase blood flow in the legs, which helps prevent deep vein thrombosis (DVT).
- Early Mobilization and Walking: Getting the patient out of bed and walking with appropriate assistive devices (like a walker or crutches) often occurs on the first post-operative day to improve circulation and reduce stiffness.
- Isometric Strengthening Exercises: These involve contracting muscles without moving the joint, such as gluteal sets (squeezing buttocks) and quad sets (tightening thigh muscles), to maintain muscle tone without putting stress on the new joint.
- Active Range of Motion Exercises (AROM): Gentle exercises to regain motion, including heel slides (bending the knee while lying down) and hip abduction (moving the leg to the side) within safe limits.
- Positioning and Hip Precautions Education: Teaching the patient proper positioning—such as keeping a pillow between the legs to avoid adduction—to prevent dislocation, particularly in the initial weeks.
- Transfer Training: Teaching the patient how to safely move from a lying to sitting position, and from sitting to standing (sit-to-stand exercises), ensuring they do not break hip precautions (e.g., avoiding excessive flexion).
- Progressive Strengthening and Gait Training: As healing progresses, exercises advance to include straight leg raises, standing hip exercises, and eventually full weight-bearing walking to normalize gait, restore balance, and improve functional independence.