A prolapsed intervertebral disc—commonly referred to as a slipped, ruptured, or herniated disc—occurs when the inner, gel-like nucleus pulposus leaks out through a crack in the outer, tougher annulus fibrosus. This misplaced disc material can compress or cause inflammation in nearby spinal nerves, resulting in severe pain, weakness, or numbness. While often painful, approximately 90–95% of prolapsed discs resolve without surgery within a few weeks to months with Physiotherapy interventions.
- Disc Structure: Intervertebral discs act as shock absorbers between vertebrae. They consist of an outer fibrous ring (annulus) and an inner gelatinous core (nucleus).
- The Prolapse Process: When the outer ring weakens due to degeneration or trauma, the inner jelly squeezes out (herniates) into the spinal canal.
- Nerve Interaction: The leaking material contains chemical substances that cause inflammation and severe pain when they contact nearby nerve roots.
- Common Locations: Most prolapses occur in the lumbar spine (lower back), particularly at L4-L5 or L5-S1, because they bear the most weight. Cervical (neck) prolapses are less common, while thoracic (mid-back) are rare.
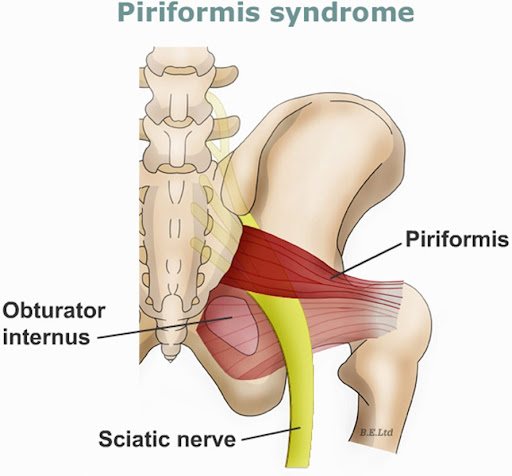
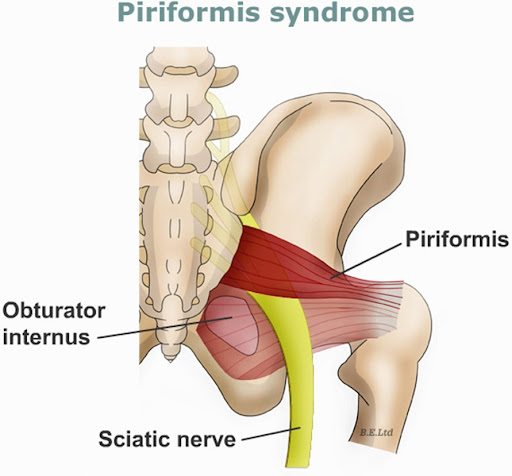
- Radicular Pain (Sciatica): Sharp, electric-shock-like pain that radiates from the back into the buttocks, legs, or feet.
- Cervical Radiculopathy: Pain radiating from the neck down to the shoulder, arm, or fingers.
- Neurological Deficits: Numbness, tingling ("pins and needles"), or muscle weakness in the affected limb.
- Mechanical Symptoms: Severe pain when bending, coughing, or sneezing.
- Cauda Equina Syndrome (Emergency): Rare but critical symptom involving bowel/bladder incontinence, numbness in the "saddle area" (groin), and progressive leg weakness.
- Degeneration: Age-related dehydration and weakening of the disc is the primary cause.
- Trauma/Injury: Sudden falls, accidents, or lifting heavy objects incorrectly.
- Repetitive Strain: Repetitive bending, twisting, or prolonged sitting/driving.
- Lifestyle: Obesity (extra load on discs), smoking (reduces oxygen supply to discs), and sedentary lifestyle.
PHYSIOTHERAPY TREATMENT
Physiotherapy for a prolapsed intervertebral disc focuses on reducing pain, centralizing symptoms, and strengthening core muscles to support the spine. Key treatments include McKenzie extension exercises, nerve mobilization, core stabilization, and manual therapy to restore function. Early intervention aims to prevent further herniation and avoid surgery.
- Pain Relief & Management: Initial focus on Reducing inflammation using TENS therapy (Transcutaneous Electrical Nerve Stimulation), heat/ice packs, and gentle posture correction to minimize irritation.
- McKenzie Method (Extension Exercises): Often the primary treatment, these exercises help "centralize" the pain, pushing the disc protrusion away from the nerve root. This includes lying prone (on the stomach), prop-ups on forearms, and prone press-ups (cobra pose).
- Manual Therapy: Physiotherapists may use spinal mobilization (e.g., posterior-anterior pressure) to improve joint mobility, reduce stiffness, and decrease muscular guarding.
- Core Stabilization Exercises: Strengthening the abdominal, paraspinal, and gluteal muscles (e.g., Bird-Dog, pelvic tilts/bridges) improves spinal stability and reduces load on the discs.
- Nerve Mobilization: Techniques to reduce neural tension in the sciatic nerve, often employing specific stretches to improve mobility and reduce leg pain.
- Postural Training: Education on proper sitting, standing, and lifting techniques to avoid increasing intradiscal pressure.
- Acute Phase: Pain reduction, minimizing nerve inflammation, and gentle mobility.
- Subacute/Rehabilitation Phase: Restoring range of motion, initiating core strengthening, and improving posture.
- Chronic/Functional Phase: Returning to daily activities, long-term stabilization, and preventing recurrence.
CONTACT US FOR A TAILORED PHYSIOTHERAPY TREATMENT PLAN. 0714673810