Piriformis Syndrome

Definition
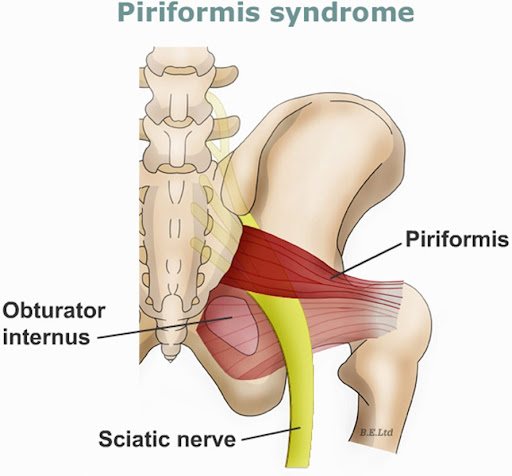
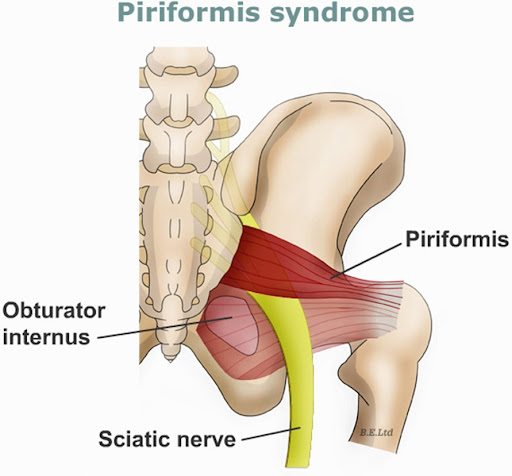
Piriformis syndrome is a rare neuromuscular disorder characterized by compression or irritation of the sciatic nerve by the piriformis muscle, causing pain, tingling, and numbness in the buttocks and down the back of the leg, mimicking sciatica. It is considered a diagnosis of exclusion, meaning other causes of sciatic nerve compression (e.g., lumbar disc herniation, spinal stenosis) must be ruled out first.
Pathophysiology
The piriformis muscle is a flat, band-like muscle located deep in the buttock, originating from the sacrum and inserting onto the greater trochanter of the femur. It primarily functions as an external rotator of the hip when the hip is extended, and an abductor when the hip is flexed. The sciatic nerve typically passes beneath the piriformis muscle, but anatomical variations exist where the nerve (or parts of it) may pass through the muscle belly.
The pathophysiology involves:
1. Piriformis Muscle Dysfunction:This can result from trauma (e.g., direct buttock trauma, fall), overuse (e.g., prolonged sitting, running, cycling), or anatomical abnormalities (e.g., hypertrophied piriformis, variations in sciatic nerve course).
2. Inflammation and Spasm:Injury or overuse can lead to inflammation, spasm, or contracture of the piriformis muscle.
3. Sciatic Nerve Compression:The inflamed, spastic, or hypertrophied piriformis muscle then directly compresses or irritates the sciatic nerve, leading to characteristic symptoms. This compression can also be dynamic, worsening with certain movements or positions that stretch or contract the muscle.

6 Clinical Features
1. Deep Buttock Pain:The most common symptom, usually localized to the gluteal region, often described as a deep ache.
2. Sciatic-like Pain:Pain often radiates down the posterior thigh and calf, sometimes into the foot, mimicking lumbar radiculopathy, but without specific dermatomal or myotomal patterns typical of nerve root compression.
3. Aggravation by Sitting:Pain typically worsens with prolonged sitting, especially on hard surfaces, and may be exacerbated by sitting with crossed legs.
4. Aggravation by Activity:Pain can be exacerbated by activities involving hip external rotation or abduction against resistance, walking, running, or stair climbing.
5. Tenderness on Palpation:Localized tenderness can be elicited upon deep palpation of the piriformis muscle over the greater sciatic notch or within the gluteal region.
6. Limited or Painful Hip Internal Rotation:Passive internal rotation of the hip with adduction often elicits or exacerbates buttock pain due to stretching of the piriformis muscle and subsequent compression of the sciatic nerve.
Examination
Clinical examination for piriformis syndrome involves:
· History:Eliciting the characteristic symptoms, aggravating/alleviating factors, and ruling out a history of low back pain or specific neurological deficits.
· Observation:Assessing posture, gait (may be normal or subtle antalgic).
· Palpation:Deep palpation in the region of the greater sciatic notch to identify tenderness over the piriformis muscle.
· Range of Motion (ROM):Assessing hip active and passive ROM, often revealing pain or restriction with passive internal rotation. Pain may also be present with resisted external rotation and abduction.
· Neurological Examination:A thorough examination of sensation, motor strength, and reflexes in the lower extremities is crucial to rule out lumbar radiculopathy. In piriformis syndrome, motor strength and deep tendon reflexes are usually normal, though mild sensory changes may sometimes be present.
2 Special Tests
1. FAIR Test (Flexion, Adduction, Internal Rotation Test):The patient lies supine. The affected hip is passively flexed to 60-90 degrees, then maximally adducted and internally rotated. A positive test is indicated by the reproduction of buttock pain and/or sciatic symptoms, suggesting the piriformis muscle is compressing the sciatic nerve in this stretched position.
2. Pace Test (Resisted External Rotator Test):The patient is seated with hips and knees flexed to 90 degrees. The examiner asks the patient to abduct and externally rotate the thigh while applying resistance to the outside of the knee. Reproduction of deep buttock pain indicates a positive test, suggesting piriformis muscle spasm or irritation.
10 Physiotherapy Interventions
1. Soft Tissue Release/Manual Therapy:Techniques such as deep tissue massage, myofascial release, and trigger point release applied directly to the piriformis muscle and surrounding gluteal musculature to reduce spasm and tenderness.
2. Stretching Exercises:Specific stretches for the piriformis muscle (e.g., supine piriformis stretch, figure-four stretch, seated piriformis stretch) to improve muscle length and reduce compression on the sciatic nerve.
3. Strengthening Exercises:Targeting hip abductors (e.g., clamshells, side-lying leg raises), hip extensors (e.g., glute bridges), and core stabilizing muscles to improve biomechanics and reduce compensatory movements.
4. Neuromuscular Re-education:Exercises aimed at improving motor control and activation patterns of the hip and pelvic girdle muscles, especially focusing on proper gluteal activation during functional movements.
5. Modalities:Application of therapeutic modalities such as heat or ice packs to the affected area to help reduce pain, inflammation, and muscle spasm.
6. Activity Modification & Ergonomics:Educating the patient on avoiding aggravating postures and activities, such as prolonged sitting, crossing legs, or repetitive hip external rotation. Recommendations for ergonomic adjustments in daily activities.
7. Postural Correction:Addressing any underlying postural imbalances or biomechanical faults in the spine or pelvis that may contribute to piriformis muscle overload or dysfunction.
8. Patient Education:Comprehensive education on the condition, self-management strategies, the importance of adherence to exercise programs, and recognition of pain triggers.
9. Dry Needling:Application of thin needles into piriformis muscle trigger points to elicit a local twitch response, aiming to release muscle tension and reduce pain.
10. Taping (e.g., Kinesio Taping):Application of therapeutic tape to the gluteal region to facilitate piriformis relaxation, reduce muscle spasm, or provide proprioceptive feedback to support proper muscle function.
DONT TRY THIS EXERCISE UNLESS RECOMMENDED BY YOUR PHYSIOTHERAPIST>

WELCOME TO KISII PHYSIOTHERAPY CLINIC,CIC ACCREDITED>