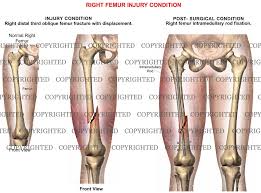
A mid-shaft femur fracture is a high-energy traumatic break occurring in the middle third of the femoral shaft, between the lesser trochanter and the femoral condyles. It involves the long, tubular part of the thighbone, often causing severe pain, deformity, and significant blood loss.

- Severe Pain in the Thigh: Immediate, acute pain concentrated in the mid-thigh area.
- Inability to Bear Weight: Patients are unable to stand or walk on the affected leg.
- Obvious Deformity/Angulation: The leg may appear bent, crooked, or shortened due to muscle pull, with the proximal segment often flexing and externally rotating.
- Significant Swelling: A tense, swollen thigh resulting from massive soft tissue swelling and bleeding.
- Substantial Hidden Blood Loss: A closed femoral shaft fracture can result in severe internal bleeding, typically losing 1,000–1,500 mL of blood.
- Bruising (Ecchymosis): Extensive bruising typically appears around the thigh and hip area.
- Crepitus/Instability: A grating sensation or sound (crepitus) or unnatural movement may be felt upon motion, which is highly painful.
- Open Wound (Open Fracture): In open fractures, bony fragments may pierce through the skin, or a puncture wound may be present.
- Radiographs (X-rays): Anteroposterior (AP) and lateral views of the full-length femur are standard.
- Joint Imaging: It is essential to obtain imaging of the hip and knee joints to detect associated ipsilateral injuries, such as a femoral neck fracture, which can accompany shaft fractures.
- Computed Tomography (CT): Used for detailed preoperative planning of comminuted or intra-articular fractures and to assess for occult fractures.
- Magnetic Resonance Imaging (MRI)/Bone Scan: Indicated if a stress fracture or pathologic (tumor-related) fracture is suspected.
- Chest Radiograph: Often performed in high-energy trauma cases to check for associated injuries.
- Physical Exam: Assessment for tenderness, swelling, and deformity, alongside a full neurovascular exam of the limb.
- Fulcrum Test: A physical exam technique specifically used to identify femoral shaft stress fractures.
- Patient History: Evaluation of the mechanism of injury (e.g., high-energy fall or car accident).
Surgical management of midshaft femur fractures typically involves intramedullary (IM) nailing, considered the gold standard for stabilizing these injuries, usually within 24–48 hours. For most cases, this provides rigid, stable fixation, enabling early mobilization. Alternatives like plating or external fixation are reserved for specific fracture types, polytrauma, or open fractures.

- Technique: A metal rod (nail) is inserted into the femoral medullary canal, acting as an internal splint to align the bone.
- Approach: Antegrade (via the hip) is common, though retrograde (via the knee) is used for specific fracture patterns or ipsilateral injuries.
- Reaming: Medullary canal reaming is often used to allow for a larger, stronger nail and to stimulate bone healing.
- Stability: Screws are inserted above and below the fracture site to prevent rotation and shortening.
- Open Reduction Internal Fixation (ORIF) with Plating: Often used when IM nailing is not possible (e.g., severe deformity, associated neck fracture) or for distal-third fractures.
- External Fixation: Used as a temporary stabilizer for open fractures or in unstable polytrauma patients (damage control orthopedics) before converting to an IM nail.

- Key Physiotherapy Interventions
- Circulatory Exercises (Ankle Pumps): Briskly bending and straightening the ankles helps maintain blood flow and prevents deep vein thrombosis (DVT).
- Isometric Quadriceps Sets: Tensing the front thigh muscles and pushing the back of the knee into the bed helps maintain muscle tone without moving the hip or knee joint.
- Gluteal Squeezes: Tightening the buttocks while lying down helps support hip stability, essential for future standing and walking.
- Heel Slides: Gently sliding the heel toward the buttocks while lying down restores range of motion (ROM) in both the hip and knee.
- Active-Assisted Range of Motion (AAROM): Using the uninjured leg or a therapist's help to move the injured leg through safe ranges of motion prevents joint stiffness.
- Straight Leg Raises (SLR): Once initial strength is regained, lifting the entire straight leg off the bed builds essential core and quadriceps strength.
- Gait Training: Learning to walk with an assistive device like a walker or crutches, progressing from non-weight-bearing to full weight-bearing as the bone heals.
- Hip Abduction Exercises: Moving the leg out to the side while standing or lying down targets the gluteus medius, which is critical for maintaining balance during walking.
- Proprioception and Balance Training: Activities like single-leg balancing (with support) help restore the body's sense of joint position, which is often lost after trauma.
- Functional Retraining (Sit-to-Stand): Practicing controlled movements like rising from a chair helps regain independence in daily activities.
VISIT US AT SANSORA NEW COMPLEX KISII TOWN OR CALL US FOR TAILORED TREATMENT AND REHABILITATION PROGRAM