Rotator Cuff Tendinitis

Pathophysiology
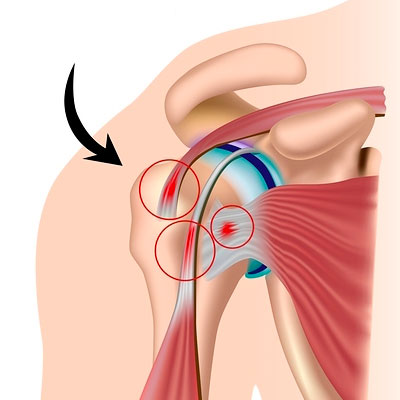
Rotator cuff tendinitis involves inflammation and irritation of the tendons of the rotator cuff muscles (Supraspinatus, Infraspinatus, Teres Minor, and Subscapularis). It typically results from repetitive microtrauma or mechanical impingement within the subacromial space. The pathology often begins with acute inflammation (tendinitis), which, if chronic, leads to tendon thickening, collagen disorganization, and vascular changes (tendinosis). The supraspinatus tendon is most commonly affected due to its location beneath the acromion and its relatively poor blood supply (the "critical zone").
Causes
· Overuse:Repetitive overhead activities (swimming, throwing, painting).
· Mechanical Impingement:Narrowing of the subacromial space due to acromial shape (hooked acromion) or subacromial spurs.
· Muscle Imbalance:Weakness in the rotator cuff or scapular stabilizers leading to superior migration of the humeral head.
· Degenerative Changes:Age-related wear and tear of the tendon fibers.
· Postural Dysfunction:Forward head and rounded shoulder posture (kyphosis).
· Trauma:Sudden strain or a fall on an outstretched arm.
Clinical Features
· Pain:Dull ache in the shoulder, often radiating to the lateral deltoid; sharp pain with overhead movement.
· Night Pain:Difficulty sleeping on the affected side.
· Painful Arc:Pain typically felt between 60° and 120° of active abduction.
· Weakness:Difficulty lifting or rotating the arm.
· Stiffness:Reduced range of motion (ROM) due to pain or secondary capsular tightness.
· Crepitus:Clicking or popping sensations during movement.
Physiotherapy Assessment and Special Tests
· Subjective Assessment:History of overhead activity, pain onset, and aggravating factors.
· Observation:Checking for muscle atrophy (supraspinatus/infraspinatus fossae) and scapular winging.
· Palpation:Tenderness over the greater tuberosity or subacromial space.
· Range of Motion:Assessing active, passive, and resisted movements.
· Special Tests:
o Neer’s Test:Passive forceful flexion of the shoulder to elicit impingement pain.
o Hawkins-Kennedy Test:Internal rotation of the shoulder at 90° of flexion.
o Empty Can (Jobe) Test:Resisted abduction in the scapular plane with internal rotation (isolates Supraspinatus).
o Drop Arm Test:Inability to slowly lower the arm from 90° abduction (indicates significant tear/tendinitis).
o Speeds Test:To rule out concurrent long head of biceps involvement.
Physiotherapy Interventions
1. Patient Education and Activity Modification:Instructing the patient to avoid provocative overhead activities and painful movements during the acute phase.
2. Pain Management (Cryotherapy):Applying ice packs for 15-20 minutes to reduce acute inflammation and numb the area.
3. Manual Therapy (Joint Mobilizations):Posterior and inferior glides of the glenohumeral joint to improve joint mechanics and decrease impingement.
4. Soft Tissue Massage:Releasing trigger points in the upper trapezius, levator scapulae, and pectoralis minor to improve scapular mobility.
5. Range of Motion Exercises:Implementing Codman’s (Pendulum) exercises to maintain joint mobility without active muscle contraction.
6. Scapular Stabilization Exercises:Strengthening the serratus anterior and lower trapezius (e.g., Scapular Squeezes, Wall Push-ups) to ensure a stable base for the cuff.
7. Isometric Strengthening:Pain-free submaximal isometric contractions for internal and external rotation to prevent muscle atrophy.
8. Progressive Isotonic Strengthening:Using resistance bands or light weights for external and internal rotation (e.g., "Side-lying ER") to build tendon load tolerance.
9. Postural Correction:Strengthening the deep neck flexors and stretching the chest muscles (Pectoralis stretch) to correct rounded shoulder posture.
10. Proprioceptive Training:Closed kinetic chain exercises (e.g., quadruped weight-shifting) to improve neuromuscular control of the shoulder complex.