Parkinson’s disease (PD) is a progressive brain condition that causes motor, mental health, sleep, and pain problems, with symptoms worsening over time. It is primarily a neurodegenerative disorder affecting dopamine-producing neurons, characterized by symptoms like tremors, stiffness, slow movement (bradykinesia), and postural instability.A neurodegenerative disorder characterized by a reduction in dopamine-producing neurons, primarily affecting movement, but also causing non-motor symptoms.
Parkinson's disease (PD) pathophysiology involves the progressive loss of dopaminergic neurons in the substantia nigra pars compacta and the accumulation of misfolded apha synuclein protein, forming Lewy bodies. This neurodegeneration, driven by mitochondrial dysfunction and neuroinflammation, leads to severe dopamine depletion in the striatum, disrupting motor circuits and causing characteristic motor symptoms.
- Dopaminergic Neuron Loss: The hallmark is the degeneration of dopaminergic neurons in the substantia nigra (midbrain), reducing dopamine availability in the striatum.
- Lewy Bodies and -Synuclein: Misfolded-synuclein protein aggregates to form intracellular inclusions known as Lewy bodies. These aggregates are thought to spread between cells in a prion-like manner, damaging neurons.
- Mitochondrial Dysfunction: Impaired energy production in mitochondria causes significant cellular oxidative stress and damage, contributing to cell death.
- Neuroinflammation: Microglia and astrocytes are activated by aggregated -synuclein, causing an inflammatory response that injures neurons.
- Dysfunctional Protein Clearance: Proteasomal abnormalities and lysosomal dysfunction hinder the cell's ability to clear toxic proteins, leading to protein buildup.

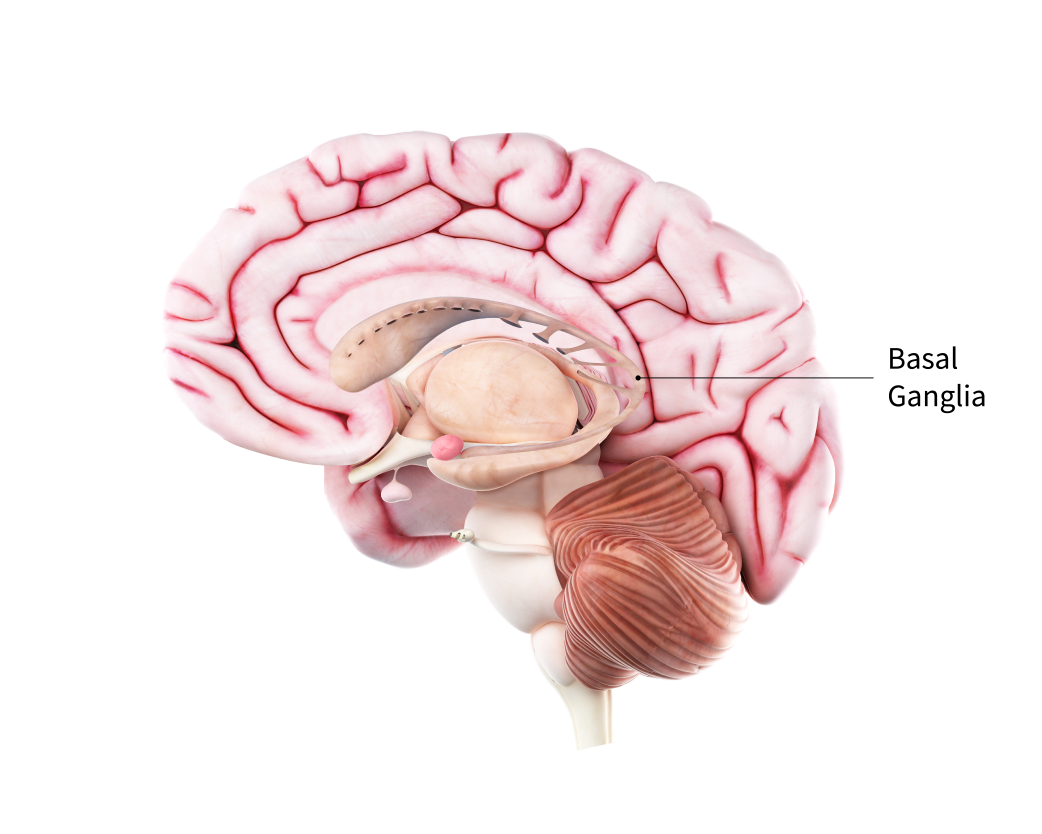
- Basal Ganglia Imbalance: Dopamine loss disrupts the balance between the direct (facilitating) and indirect (inhibiting) motor pathways, resulting in bradykinesia, rigidity, and tremor.
- Reduced Receptor Density: Dopamine depletion leads to changes in the density and sensitivity of dopamine receptors within the striatum.
- Non-motor Impacts: Beyond the dopamine system, the neurodegenerative process affects norepinephrine, serotonin, and acetylcholine systems, contributing to non-motor symptoms like dementia and autonomic dysfunction.

CAUSES
Parkinson's disease is caused by a loss of nerve cells in the part of the brain called the substantia nigra. Nerve cells in this part of the brain are responsible for producing a chemical called dopamine.
- 3.Rigidity (Muscle Stiffness): Stiffness or tightness in the limbs, neck, or trunk, which can cause pain and restrict range of motion. It is often described as "cogwheel rigidity" (a ratchet-like resistance during movement).
- 4.Postural Instability (Balance Problems): Difficulty maintaining an upright, steady posture, often leading to a high risk of falls. This usually develops in the middle or later stages of the condition.
- 5.Shuffling Gait (Walking Difficulties): A characteristic walking style involving small, shuffling steps with reduced or no arm swing. It may also include "freezing," where the feet feel glued to the floor.
- 6.Masked Face (Hypomimia): A reduction in facial expressions, causing a person to appear serious, depressed, or uninterested, even when they are not. It is caused by the stiffening of facial muscles.
- 7.Micrographia (Small Handwriting): A change in handwriting that becomes noticeably smaller, cramped, and crowded as the disease progresses.
- 8.Hypophonia (Soft Voice): A decrease in the volume and tone of the voice, often resulting in a soft, monotone, or breathy speaking style.

- History Taking: Review medication timing (on/off times), history of falls, and patient-specific goals.
- Postural Assessment: Observation for stooped posture, scoliosis, or neck flexion.
- Movement Analysis (Motor Function):
- Bradykinesia: Evaluated via finger tapping, hand grip, and rapid alternating movements (e.g., pronation/supination) to assess speed and amplitude reduction.
- Rigidity: Assessed through passive range of motion, looking for "lead pipe" or "cogwheel" resistance in limbs.
- Tremor: Observation of resting tremor, often described as "pill-rolling".
- Functional Mobility & Gait:
- Gait Analysis: Evaluating walking speed, shuffling, arm swing, and turning.
- Freezing of Gait (FOG): Assessing for gait initiation failure or "magnetic" feet.
- Transfers: Assessing ability to get out of a chair or turn in bed.
- Balance & Falls Risk:
- Berg Balance Scale (BBS): A widely used, comprehensive measure of balance.
- Timed Up and Go (TUG): Measures mobility and fall risk.
- Five Times Sit-to-Stand (5TSTS): Assesses functional lower limb strength.
- Strength and Endurance: Assessment of muscle weakness, particularly in antigravity muscles and core.
- Key Assessment Tools
- Lindop Parkinson’s Assessment Scale (LPAS): Specifically designed to measure functional decline in PD.
- Ten-Meter Walk Test: To measure walking speed.
- Freezing of Gait Questionnaire: Used to assess the severity of freezing episodes.
- Functional FocusThe assessment identifies how symptoms interfere with daily living, such as navigating tight spaces or rising from a chair, allowing the physiotherapist to tailor exercise programs focusing on cueing strategies, flexibility, and strengthening.PHYSIOTHERAPY MANAGEMENTPhysiotherapy management for Parkinsonism aims to improve functional independence, mobility, and safety by addressing rigidity, bradykinesia, and balance issues through tailored exercise. Key strategies include treadmill training, high-intensity aerobic exercise, strengthening, and cueing techniques to enhance movement quality, reduce falls, and improve quality of life.Here are 10 key physiotherapy management techniques in Parkinsonism:
- Gait Training and Cueing Strategies: Use auditory (rhythmic music/metronome), visual (laser lines, floor markers), or proprioceptive cues to reduce freezing of gait and improve stride length.
- Amplitude-Focused Training (BIG Therapy): Exercises designed to counteract bradykinesia (slow movement) by exaggerating movement amplitude, encouraging large, forceful movements in all rehabilitation activities.
- Progressive Resistance Training: Strengthens major muscle groups (quadriceps, hip extensors, upper limbs) to counteract muscle atrophy, improve posture, and improve functional mobility.
- Balance Training and Fall Prevention: Specific exercises on uneven surfaces, single-leg stands, and perturbation training to improve stability and prevent falls.
- Aerobic Exercise: High-intensity training (e.g., stationary cycling, fast walking, swimming) increases aerobic capacity, enhances mobility, and may have neuroprotective benefits.
- Flexibility and Mobility Exercises: Dedicated stretching routines, especially targeting the hip flexors, hamstrings, and pectoral muscles, to alleviate rigidity and prevent contractures.
- Dual-Task Training: Training the patient to perform cognitive (counting backward) or motor tasks (holding an object) while walking to improve safety during daily living activities.
- Functional Task Training (Transfer Training): Targeted exercises for specific deficits, including improving bed mobility (turning) and rising from a chair or floor.
- Postural Correction Exercises: Strategies to address "bent" posture (kyphosis) through axial mobility exercises and spinal extension techniques to maintain upright posture.
- Breathing and Respiratory Training: Exercises to increase chest expansion, improve expiratory effort, and manage respiratory complications related to muscle rigidity.
Rehabilitation Strategies- Early Referral: Early diagnosis and immediate physiotherapy intervention can prevent long-term functional decline.
- Multidisciplinary Approach: Collaboration with neurologists and occupational therapists for holistic management.
- Home Exercise Programs: Promoting consistent, long-term home-based exercises to maintain gains achieved during therapy sessions.
CONTACT A QUALIFIED PHYSIOTHERAPIST FOR BEST OUTCOMES IN PARKINSONISM.