- Rapid Onset: Symptoms appear suddenly, often including weakness, numbness, speech difficulties, or visual issues.
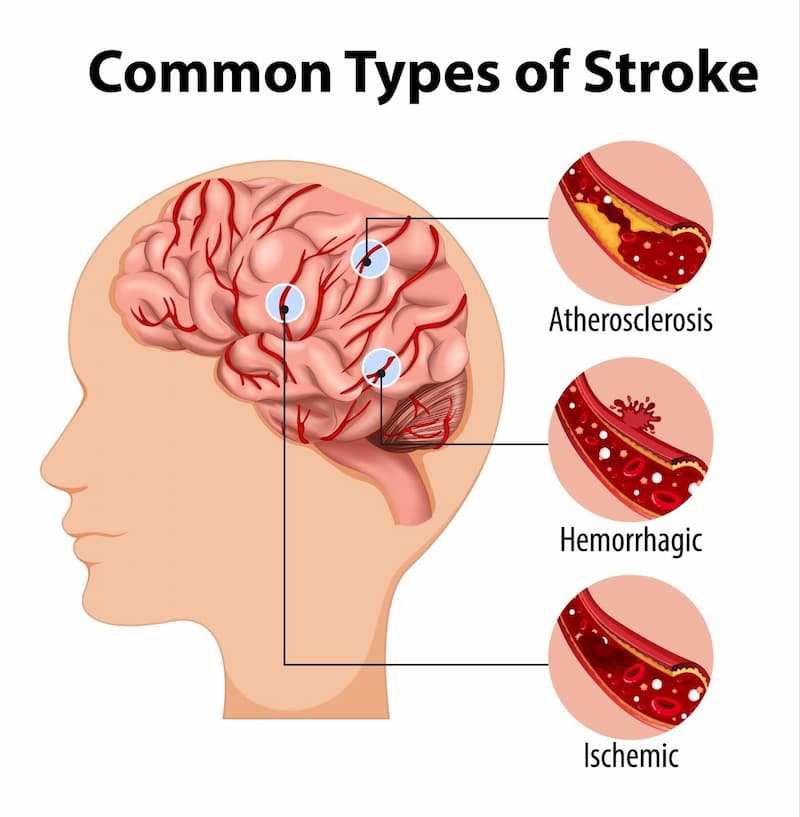
- Vascular Origin: The damage is caused by a disruption in blood supply to the brain, such as a blockage (ischaemic stroke) or a burst vessel (haemorrhagic stroke).
- Duration: Symptoms last 24 hours or longer, or lead to death.
- Disturbance Type: Includes focal or global disturbances of cerebral function.

- Haemorrhagic Stroke: Caused by a ruptured blood vessel leading to bleeding in the brain.
- Transient Ischaemic Attack (TIA): While a TIA typically lasts less than 24 hours and is considered a "mini-stroke," the overall definition of stroke involves lasting damage.
- Balance: Sudden loss of balance, coordination, or dizziness.
- Eyes: Sudden vision changes, blurred vision, or trouble seeing in one or both eyes.
- Face:An uneven smile, facial drooping, or numbness on one side.
Management / Interventions
Early Management of Acute Stroke
The goal for the acute management of patients with stroke is to stabilize the patient and to complete initial evaluation and assessment, including imaging and laboratory studies, within a short time frame. Critical decisions focus on the need for intubation, blood pressure control, and determination of risk/benefit for thrombolytic intervention.[10]
Patients presenting with Glasgow Coma Scale scores of 8 or less or rapidly decreasing Glasgow Coma Scale scores, require emergent airway control via intubation.
A recent study has shown gait improvement with high-intensity interval training and moderate-intensity continuous training in ambulatory chronic stroke patients. According to post-stroke guidelines, moderate-intensity, continuous aerobic training (MCT) improves aerobic capacity and mobility after stroke. High-intensity interval training (HIT) has been shown to be more effective than MCT among healthy adults and people with heart disease.
Physiotherapy

Physiotherapists should be involved early and should make their own assessment of how much they can work with a patient. Early mobilisation is associated with better outcomes - even after taking account of the potential confounding influence of disease severity. If rehabilitation is to take place on a different ward from acute care, the care received should be made as seamless as possible. The type and intensity of therapy should be determined by the patient's needs, not location.Physical exercise acts as prototypical preconditioning stimuli that offer brain protection effects and are safe and workable treatment options for providing endogenous neuroprotection in patients with acute and chronic stroke.
Age, arm paresis, aphasia, and facial palsy at index stroke were predictors of increased muscle tone seven years post-ischaemic stroke. A randomized study examining the effects of balance training with electromyogram-triggered functional electrical stimulation (EMG-triggered FES) to improve static balance, dynamic balance, and ankle muscle activation suggest positive results with stroke patients.
Positive outcomes with self-initiated sit-to-stand training on speeding up regaining the independence of sit-to-stand on sub-acute stroke survivors. A Systematic Review suggests that only lifestyle interventions that include specific strategies targeting physical activity have a positive outcome on physical activity levels as compared to general lifestyle interventions.
Primary Goals of Rehabilitation
- Prevent complications
- Minimise impairments
- Maximise function
Optimising Post Stroke Rehabilitation
- Early assessment with standardized evaluations and validated assessment tools
- Early employment of evidence-based interventions relevant to individual patient needs
- Patient access to an experienced multidisciplinary rehabilitation team
- ongoing medical management of risk factors and co-morbidities
A randomized controlled trial suggests the CARE4STROKE program had a positive outcome on anxiety and depression of the patients.
Upper Limb
Upper Limb Impairments:
- Subluxation
- Changes in Sensation
- Contracture
- Swelling
- Coordination Problems
- Weakness
- Altered Muscle Power
- Changes in Muscle Tone
- Hand Dysfunction
Aims of Treatment:- Prevent shoulder pain and if unable to do so, manage should pain effectively.
- Be selective when choosing compensatory versus remedial intervention methods to treat clients who are predicted to have a low return of motor function and poor functional use of their arm and hand.
- Provide remedially focused rehabilitation to clients who are predicted to change in arm and hand function.
- Use measures of known reliability and evidence of validity for treatment planning and outcome prediction.
In the upper extremity with severe impairment and/or poor prognosis for recovery (Chedoke McMaster Stroke Assessment (CMSA) of Arm and Hand < Stage 4) treatment should focus on maintaining a comfortable, pain-free, mobile arm and hand.
- Focus on proper positioning to provide support at rest and careful handling during functional activities
- Participate in classes supervised by professional rehabilitation clinicians in institutional or community settings that teach the client and caregiver to perform a self range of motion exercises.
- Avoid the use of overhead pulleys (risk of shoulder tissue injury)
- Use some means of external support for stage 1 or 2 upper limbs during transfers and mobility
- Place arm and hand in a variety of positions that include placement within the client’s visual field
- Use some means of external support to protect the upper limb during wheelchair use
In the upper extremity with moderate impairments who show high motivation and potential for functional motor gains (CMSA => stage 4)
- Engage in repetitive and intense use of novel tasks that challenge the stroke survivor to acquire necessary motor skills to use the involved upper limb during functional tasks and activities
- Engage in motor-learning training including the use of imagery.
Treatment Techniques:
- Strength Training - There is evidence that strength training can improve upper-limb strength and function without increasing tone or pain in individuals with stroke. A randomized study examining the effects of balance training with electromyogram-triggered functional electrical stimulation (EMG-triggered FES) to improve static balance, dynamic balance, and ankle muscle activation suggest positive results with stroke patients. A Randomized Controlled Trial showed improvement in strength and motor function in patients after subacute stroke with high-intensity and low-intensity arm resistance training.
- Modified Constraint-Induced Movement Therapy (mCIMT) and CIMT address learned non-use and decreased motor function in an upper extremity affected by post stroke.Performing aerobic exercise prior to m-CIMT enhances the outcomes.
- Orthotics - therapy incorporating a dynamic wrist-hand orthosis may be no better than manual therapy. Long-term use of static orthoses requires complementary appropriate treatment opportunities to prevent clenched fist, problems with ADL and hygiene maintenance.
- Gaming - goal-orientated computer gaming has proven to significantly reduce upper limb impairment in stroke survivors
- Virtual Reality - virtual reality training has been shown to be effective in restoring upper limb motor impairments and motor-related functional abilities
- Mirror Therapy - Mirror therapy has been shown to have a beneficial effect on motor control and function compared with conventional therapy
- Robot-Assisted Therapy - has been shown to have a beneficial effect on motor recovery and function.
SUMMARY OF PHYSIOTHERAPY INTERVENTIONSPhysiotherapy interventions in stroke recovery focus on regaining motor function, balance, and independence through neuroplasticity. Key interventions include early mobilization, strength training, gait training, Constraint-Induced Movement Therapy (CIMT), and mirror therapy to address weakness, spasticity, and functional limitations.- Early Mobilization: Initiated within 24-48 hours to prevent complications, involving sitting, standing, and guided movement.
- Task-Oriented Training: Repetitive practice of daily tasks (e.g., reaching, grasping, sit-to-stand) to improve functional mobility.
- Constraint-Induced Movement Therapy (CIMT): Restraining the unaffected limb to force the use of the affected upper limb.
- Strength Training: Progressive resistance exercises using bands, weights, or body weight to rebuild muscle strength.
- Balance Training: Exercises such as weight shifting, standing on one leg, and tandem walking to reduce fall risk.
- Gait Training: Treadmill training (with or without body weight support) and overground walking to retrain walking patterns.
- Mirror Therapy: Using a mirror to create an illusion of movement in the affected limb, stimulating brain recovery.
- Functional Electrical Stimulation (FES): Using electrical currents to stimulate muscles for movement, often used for foot drop or shoulder subluxation.
- Robot-Assisted Therapy: Using robotic devices for intensive, high-repetition therapy of the arms or legs.
- Spasticity Management (Stretching/Positioning): Sustained stretching and proper positioning to manage muscle tightness and prevent contractures.
ALWAYS ENGAGE A QUALIFIED PHYSIOTHERAPIST TO AVOID RISKING THE LIFE OF A PATIENT.